

Clinician Resources
ASTMH guidance on clinical laboratories offering testing for parasitic diseases: https://www.astmh.org/education-resources/CDC-Alternative-Lab-Tests

Items to address before prescribing benznidazole or nifurtimox
Have a patient with Chagas disease who needs treatment? Before prescribing benznidazole or nifurtimox, review this helpful guidance document.

Benznidazole
Learn how to prescribe benznidazole in the US.
Atendiendo Chagas
Mundo Sano’s “Atendiendo Chagas” Network is a global network of Chagas disease healthcare providers, researchers, and other professionals. To join this international group, please follow this link: https://atendiendochagas.mundosano.org/registrarse

CDC Course: What US clinicians need to know about Chagas disease
Free online module to educate clinicians about Chagas Disease in the US.
CDC Course: Optimizing Chagas care for pregnant women and children
Free online module congenital to educate US clinicians on congenital Chagas disease practices and strategies

CDC DPDx: Trypanosoma cruzi
Information on laboratory diagnosis of T. cruzi and photos of T. cruzi and triatomine vectors

Lampit (nifurtimox) received FDA approval on August 6, 2020
Please see Lampit.com for additional information.
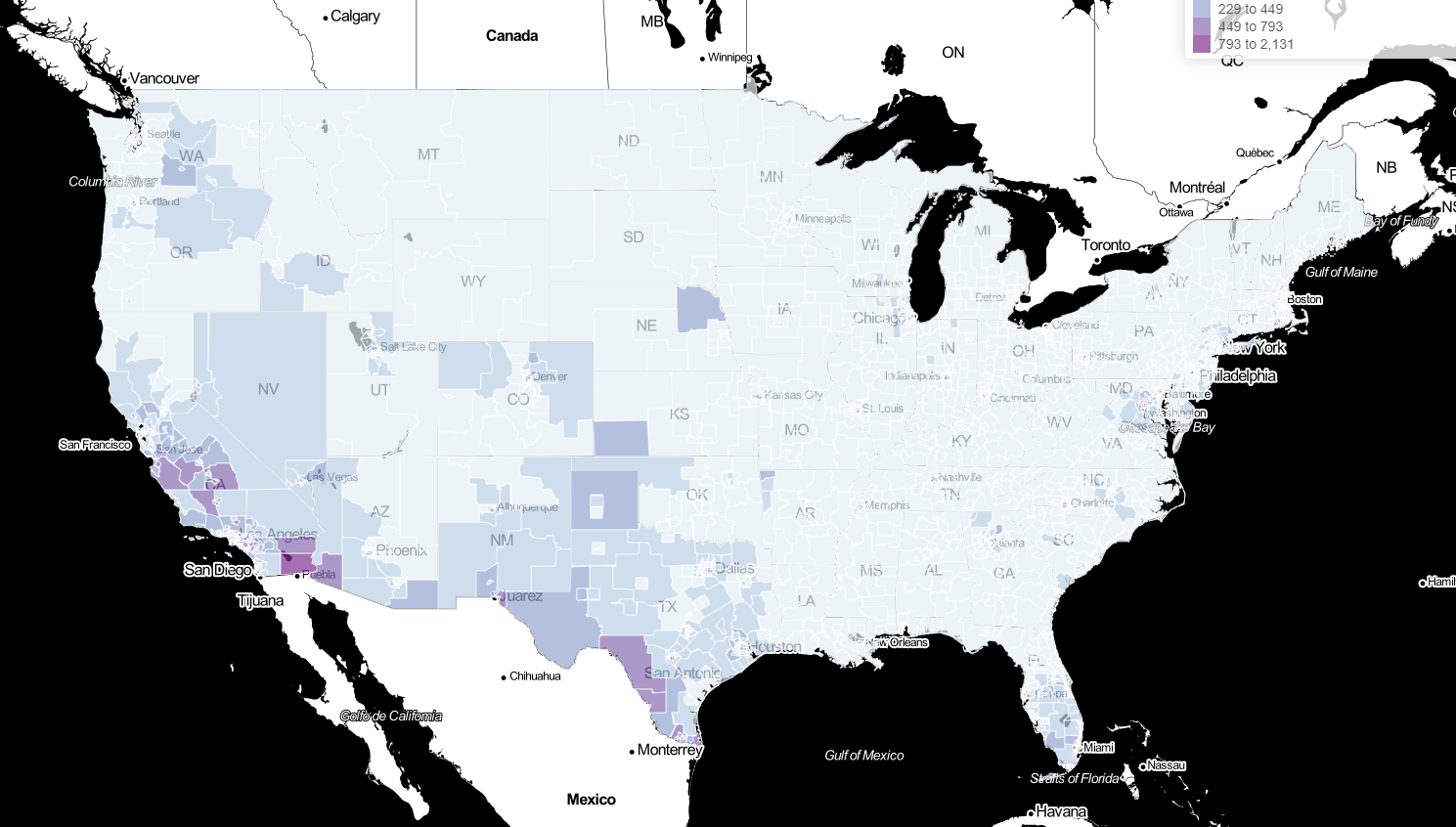
Updated Estimates and Mapping for Prevalence of Chagas Disease among Adults, United States
Map 1 - Number of T. cruzi infections in adults
Map 2 - Percent of adult population with T. cruzi infections
Map 3 - Percent of adult Latin American-born population with T. cruzi infections